HDRN Canada has strong showing at CAHSPR 2025


HDRN Canada had a strong showing at the Canadian Association for Health Services and Policy Research annual conference in Ottawa last month, highlighting network developments following this year’s theme, “charting the course for health system transformation.”
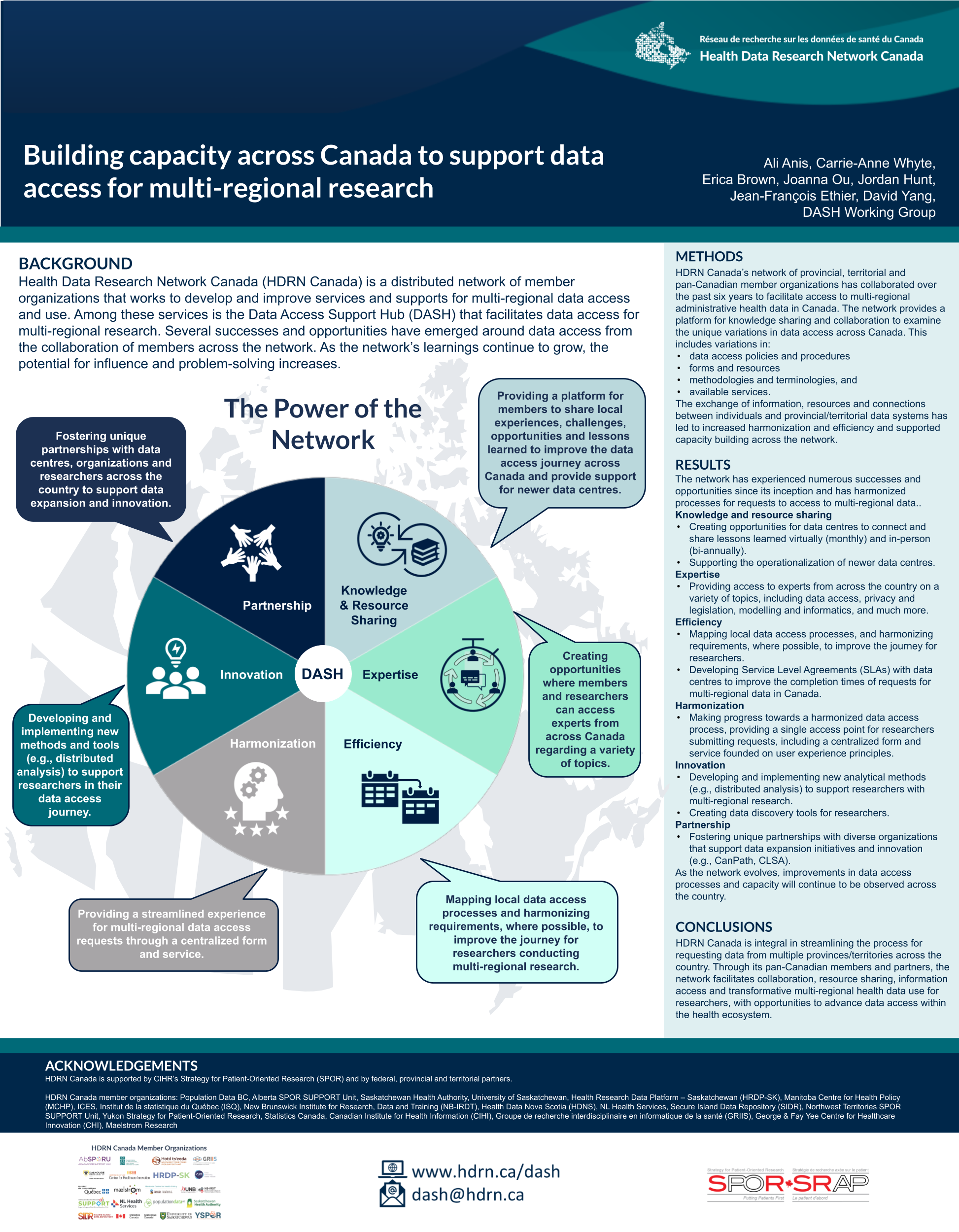
The DASH Team showcased successes and opportunities that emerged through a collaboration of HDRN Canada’s network of pan-Canadian member organizations in building the Data Access Support Hub (DASH) service. DASH is a one-stop shop for researchers seeking access to multi-regional population-based health data in Canada. A poster presented by Carrie-Anne Whyte, DASH Program Lead, highlighted how advancements developed across the network are made available to researchers through DASH.
{kind=link}
Technological innovation in distributed analysis and the creation of data discovery tools are huge advantages for researchers ~ Carrie-Anne Whyte
“Technological innovation in distributed analysis and the creation of data discovery tools are huge advantages for researchers,” she said. Other improvements like increased harmonization and efficiency in the DASH service were made possible through collaborative capacity building, sharing resources and exchanging knowledge around unique variations in data access across Canada, she noted. “Fostering data expansion initiatives with partners like CanPath and the Canadian Longitudinal Study on Aging have also been critical for expanding our data offerings and linkage,” Whyte said.
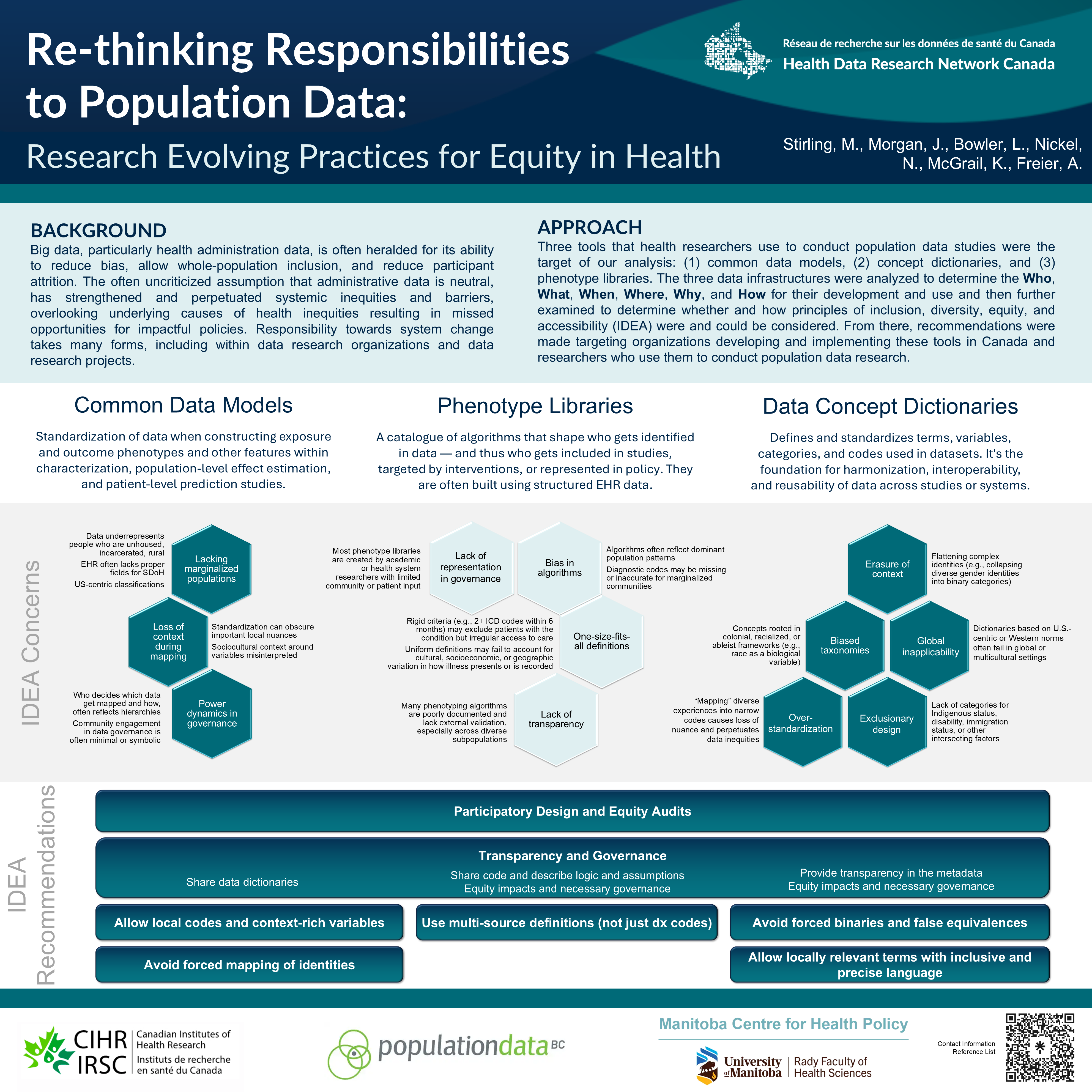
The harmful assumption that routinely collected health data are neutral, resulting in the perpetuation of systemic inequities, was the focus of a poster presented by the IDEA Team‘s Dr. Laura Bowler. This work examined three tools used to conduct population data studies: common data models, phenotype libraries and data concept dictionaries. “We wanted to understand how and why data research organizations and health researchers bear responsibility for system change,” Dr. Bowler explained. Many concerns regarding inclusion, diversity, equity and accessibility emerged in the analysis of these tools, and recommendations for organizations developing and implementing these tools as well as researchers using them included participatory design, equity audits, transparency and governance.”
{kind=link}
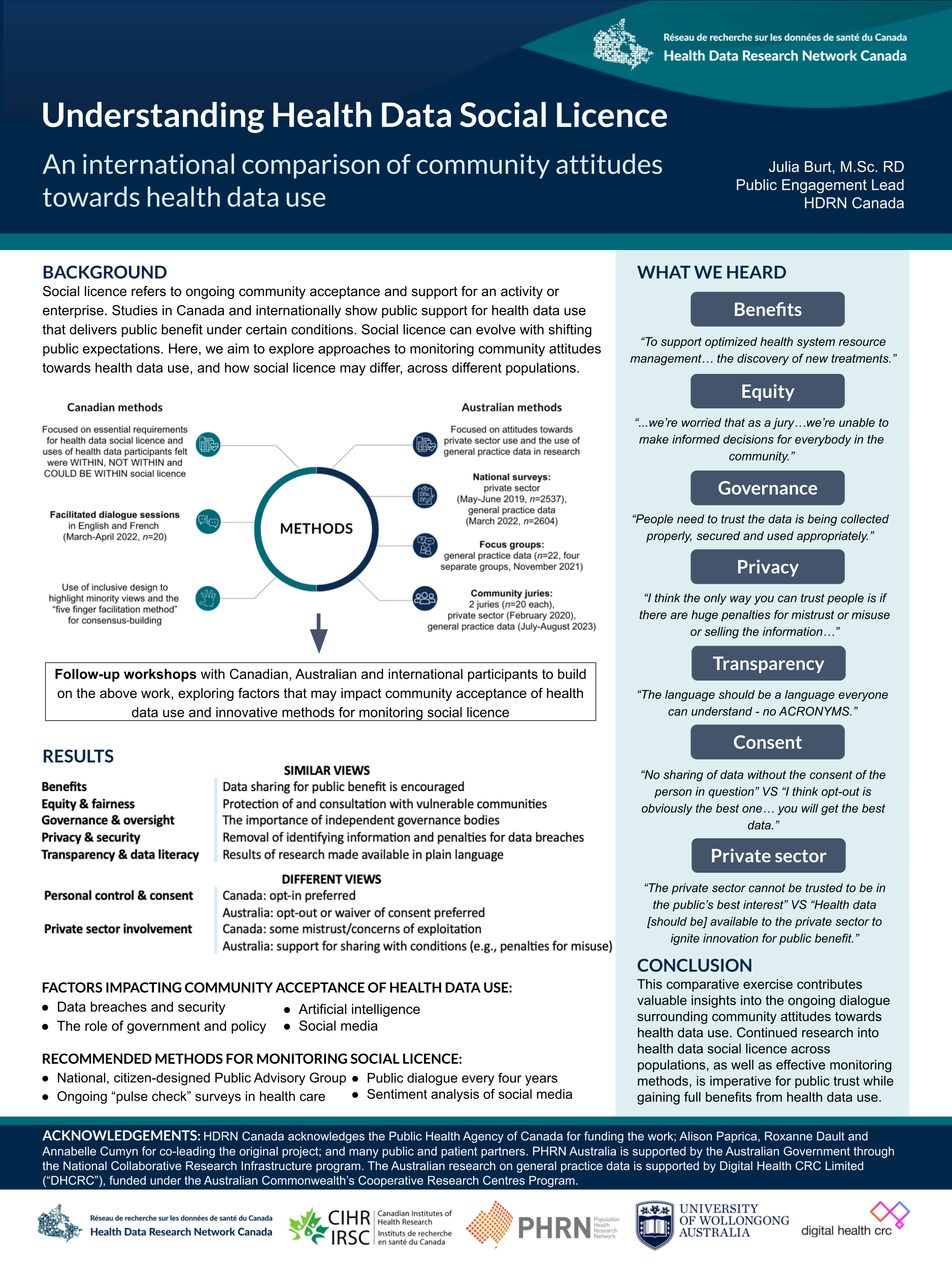
To understand acceptable uses of health data, a poster from the Public Engagement Team compared public perspectives in Canada and Australia. It featured a collaboration with Australia’s Population Health Research Network, an HDRN Canada partner, that examined community attitudes towards “social licence” for health data use. They found that data sharing for public benefit is encouraged in both countries, as is protecting and consulting with vulnerable communities. Independent governance and penalties for data breaches were also priorities shared in both countries. The collaboration will continue, said Julia Burt, Public Engagement Lead: “Continued research into health data social licence across populations, as well as effective monitoring methods, is imperative for public trust while gaining full benefits from health data.”
{kind=link}
In her oral presentation, Dr. Lisa Lix, Lead of the Algorithms and Harmonized Data Team, shared developments in ongoing work to protect personally identifiable information contained in electronic medical records (EMRs) so those records can be safely included in critical health research. Three HDRN Canada member organization data centres are participating in a pilot study to implement a machine-learning de-identification algorithm for free text found in EMRs.
“The de-identification algorithm is trained to redact, mask or retain potentially sensitive information. To date, we have documented the differences in provincial privacy legislation, trained annotators from all centres, and developed appropriate criteria to annotate the EMRs that will be used to train the algorithm and evaluate its performance,” Dr. Lix said. “Next steps will be to use the annotated data with the de-identification machine-learning algorithm to produce site-specific accuracy estimates in an iterative process. With appropriate approvals from data custodians at each site, we will then implement federated learning algorithms across all three data centres.”
Julia Burt’s oral presentation, Public Trust, Literacy and Health Data Foundations in Canada, shared a collaboration with the Public Health Agency of Canada exploring the critical importance of public trust in health data use and the role of data literacy as an essential precondition. The paper draws upon three online focus groups, four key informant interviews and a survey completed by more than 60 respondents, as well as a literature review. “The findings affirmed previous work,” commented Burt. “Increased trust in health data use supports health system planning and innovation. But the risks of health data use, like stigmatization and harm to communities, impede trust.” The new contribution of this paper was the development of six principles-based recommendations for trustworthy health data practices.
Register for our upcoming webinar Public Trust, Literacy and Health Data Foundations in Canada, taking place THURSDAY, JUNE 26 online.